

By Frangiska Mylona,
The heart is one of the most significant organs not only in the human body but for every organism that contains a heart or a primitive heart structure. It has one very simple but crucial function; to pump blood throughout the body. Anatomically, it is made of four chambers; two atria where there is one on the left side and one on the right side, and two ventricles, located below the two atria, with, again, one on each side. The atria are separated from the respective ventricles through the valves. The tricuspid valve separates the right atrium from the right ventricle while the mitral valve separates the left atrium from the left ventricle. The valves ensure that there will be no backflow of blood as it is pumped from the atria to the ventricles. Additionally, the atria and ventricles are separated from one another by septa; the interatrial septum isolates the two atria from each other, and the interventricular septum with its membranous and muscular parts separates the two ventricles from each other. Also, another septum is observed, the atrioventricular septum separating the atria from the ventricles.
As it is understood, the function of the atria is to collect blood while the main function of the ventricles is to expel blood. The right atrium receives deoxygenated blood from the systemic venous circulation from the superior and inferior venae cavae. Then, it sends it to the right ventricle which will pump the blood to the pulmonary artery and eventually this blood will enter the lungs. On the other hand, the left atrium receives oxygenated blood from the lungs via the pulmonary veins and sends it to the left ventricle for the ventricle to pump it to the aorta and from there this blood will reach the rest of the body through the systematic circulation.
The same valvular division, that separates the atria from their respective ventricles, applies to the ventricles with their respective outflow vessels. Therefore, the right ventricle is separated from the pulmonary artery via the pulmonary valve while the left ventricle is separated from the aorta by the aortic valve. The pumping of blood is based on the events of the cardiac cycle which includes the well-known concepts of diastole and systole.
In order for the heart to be able to pump this blood, it needs some electrical activity to be generated. This will ensure that the atria and the ventricles will contract to send the blood to its multiple destinations and fulfill the body’s needs. There is something fascinating about this hollow muscular organ. It is composed of two types of cardiac myocytes: conducting and contractile. Conducting cardiomyocytes have the ability to generate an impulse or, in other words, an action potential that will stimulate the heart to contract. In this type of cell, action potentials are generated without the interference of the sympathetic nervous system, which is known as automaticity. However, the automaticity can be influenced by the sympathetic and parasympathetic nervous systems, from certain types of drugs, stress, the metabolic activity of the body, the electrolyte levels, etc… After this impulse is generated, the other type of cells, the contractile cells, will start to contract as a response to this type of signal.
There are five places where conducting cardiomyocytes are found in the heart:
1) The SA or the sinoatrial node where is located in the right atrium. It is the heart’s natural pacemaker since it reaches the threshold potential for the generation of an action potential the fastest. It generates beats with a 60-100 bpm rhythm. From there the action potential travels to both the atria via junctions known as gap junctions and to the atrioventricular or AV node.
2) As it is mentioned above, the next place that the action potential will travel to, is the AV node. It is located in the atrioventricular septum and it delays the process of propagation of the action potential to the ventricles. This happens so that the atria will have enough time to fill the ventricles with blood.
3) Action potentials travel from the AV node to the bundle of His, made up of a complex organization of cells that eventually will spread the action potential to the bundle branches. The bundle of His is located in the membranous part of the interventricular septum.
4) The bundle branches are divided into left and right bundle branches to ensure that the action potential will reach both the right and left ventricles simultaneously.
5) Lastly, the action potential will reach a network of special fibers, the Purkinje fibers that are located through the ventricular walls.
To ensure proper blood pumping, the action potential causes simultaneous contraction of both atria and ventricles. It is important to note that all of these five nodes have the ability to initiate an action potential. However, the SA node is the natural pacemaker of the heart because it reaches a threshold potential the fastest. If it is damaged, the rest of the nodes will try to compensate by generating an action potential but it will be of lower intensity.
It is important to emphasize that the action potential is generated due to the influx and efflux of critical electrolyte ions. These are the potassium, sodium, and calcium ions. That is why it is vital to check the levels of these electrolytes when a check-up is performed.
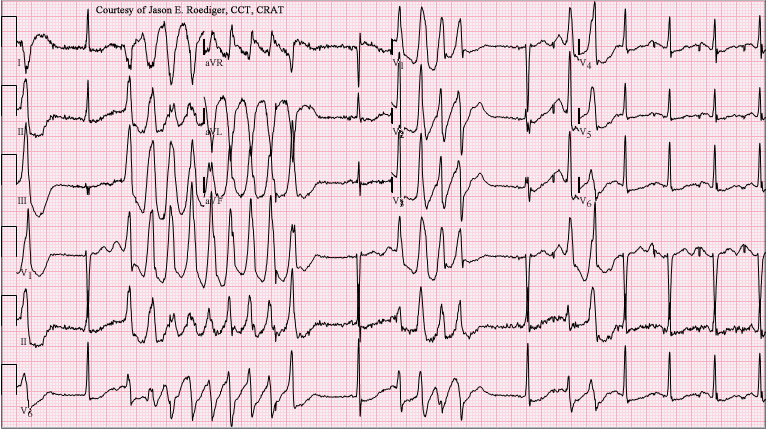
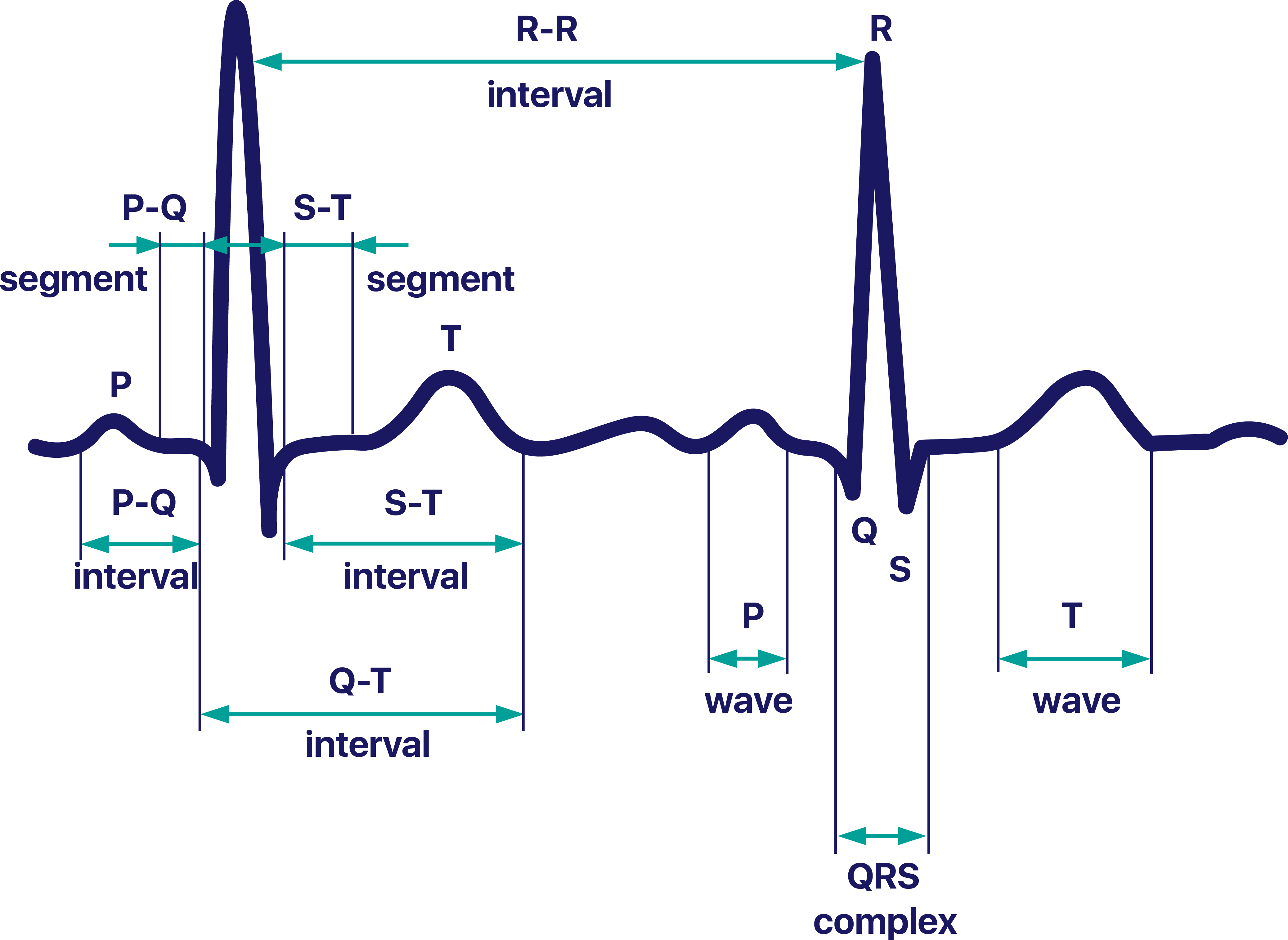
A very familiar test that depicts the journey of the action potential through the heart is the electrocardiogram, ECG for short. The ECG consists of several waves, intervals, and complexes that depict the journey of the action potential. Analytically:
A) The P wave: It represents atrial contraction
B) The PQ interval represents the time for the atrial to pump blood to the ventricles as the action potential passes to the AV node.
C) The QRS complex represents the ventricular contraction where the Q wave depicts the action potential journey from the bundle of His to the bundle branches while the RS interval represents the action potential in the Purkinje’s fibers. The QRS complex should last for less than 0.10 seconds.
D) Lastly, the T wave represents ventricular relaxation until the next action potential is fired.
The time between the PR interval should be around 0.12 to 0.2 seconds. The time between the QT interval should be less than 0.42 in men and less than 0.43 in women. Generally, there are some deviations from the normal cardiac cycle values for different groups of people. For example, in adults, a complete cardiac cycle lasts for 0.7 to 1 sec (60-100 bpm) while in well-trained athletes, it lasts for 1.2 sec (50 bpm), and in young people, it lasts for 0.6 seconds (around 100 bpm).
The condition when the heart’s electrical activity becomes abnormal, resulting in disturbances in the rate, rhythm, sequence, or origin of the conduction of an action potential, is referred to as arrhythmia.
Arrhythmia is classified as whether there is a change in the rate of tachyarrhythmias/tachycardias (more than 100 bpm) or in bradyarrhythmias/bradycardias (less than 60 bpm). The tachycardias are divided into categories according to their location supraventricular or ventricular, focal, and multifocal. Similarly, bradycardias are evaluated according to the location of the abnormal impulse and if there are any conduction blocks.
There are many mechanisms involved in the pathophysiology of arrhythmias. The mechanisms include impaired automaticity, triggered activity causing cell irritability, or reentry circuits for action potentials. Tachycardia can result from these causes, while bradycardia is caused by a conduction block or decreased automaticity.
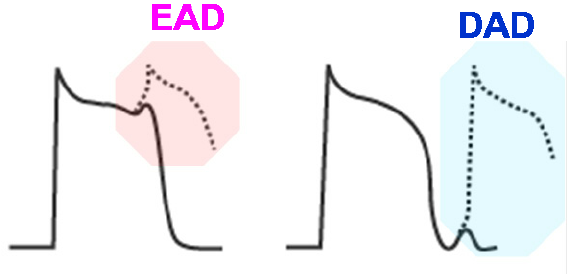
One of the most deadly tachyarrythmias is known from the french term “Torsades de pointes” it is translated as the points that “dance”. This refers to the abnormalities that are observed on the ECG. Torsades de pointes is pathophysiologically caused by triggered activity. In general, this is caused by the abnormal leakage of positive ions into cardiac cells, resulting in after-depolarizations strong enough to initiate primitive action potentials. EADs (early after depolarization) and DADs (delayed after depolarization) are two types of after-depolarizations. EADs are linked with low levels of the respective electrolytes. They are linked with both congenital conditions like hereditary disorders that affect the membrane of the ion channel proteins with either potassium or sodium channel defects that are important for the normal permeability of the electrolytes and play a crucial role in the action potential generation and also to some acquired causes like drug intoxication.
The drugs that can cause an EAD go by the acronym ABCD and are associated with class I antiarrhythmic drugs which are sodium channel blockers (IA, IB, IC) that can cause Torsades de Pointes. Also, it is associated with certain antibiotics, antipsychotic drugs, antidepressants, and antiemetics.
The morphology of this type of tachyarrhythmia is linked with the prolongation of the QT interval on the ECG which may result in this characteristic type of ventricular polymorphic tachycardia. This will result in the ECG points “dancing” or having an abnormal morphology, which will result in sudden cardiac death. Also, the QRS complexes are large, bizarre, and polymorphic that vary in amplitude and direction. The rhythm is highly unstable, ranging from 100-180 bpm or even 200-300 bpm! This rhythm may lead to ventricular fibrillation, a very dangerous situation where the ventricles instead of normally contracting, contract in a very rapid and uncoordinated manner resulting in quivering which leads to the ventricles not pumping blood to the rest of the body or to the lungs which can lead to sudden death and it requires immediate medical intervention. Again this syndrome can be caused by the above congenital and acquired causes.
The symptoms of the Torsades de pointes include dizziness and lightheadedness along with palpitations that can lead to fainting or syncope and eventually cardiac arrest and death. The diagnosis is based on the ECG and echocardiogram findings and it should be accompanied by blood tests that check the electrolyte levels. There are two types of treatment: pharmacological and surgical. The pharmacological treatment involves the intake of magnesium and even potassium as well as drugs known as β-blockers and the surgical interventions include the placement of a pacemaker, and Implantable cardioverter defibrillator (ICD).
It follows that the heart is an autonomous and intelligent organ, but it needs to be treated delicately. In order to keep us alive, it recruits so many cells and uses so many substances only to generate an action potential that allows us to seize the day once more.
References
- Porth’s Essentials of Pathophysiology, Fifth edition by Tommie L. Norris, DNS, RN and Rupa Lalchandani Tuan, Ph.D.

