

By Frangiska Mylona,
According to WHO (World Health Organization) data, cephalgia or headache, is among the top three neurological disorders for most age groups, with the epidemiological studies showing that in 2021, 40% of the population, which means around 3.1 billion people, had experienced at least once an episode of headache, with the prevalence being higher for the female than the male population.
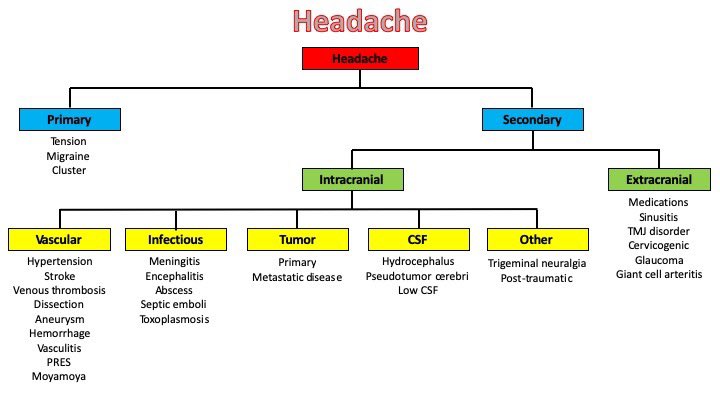
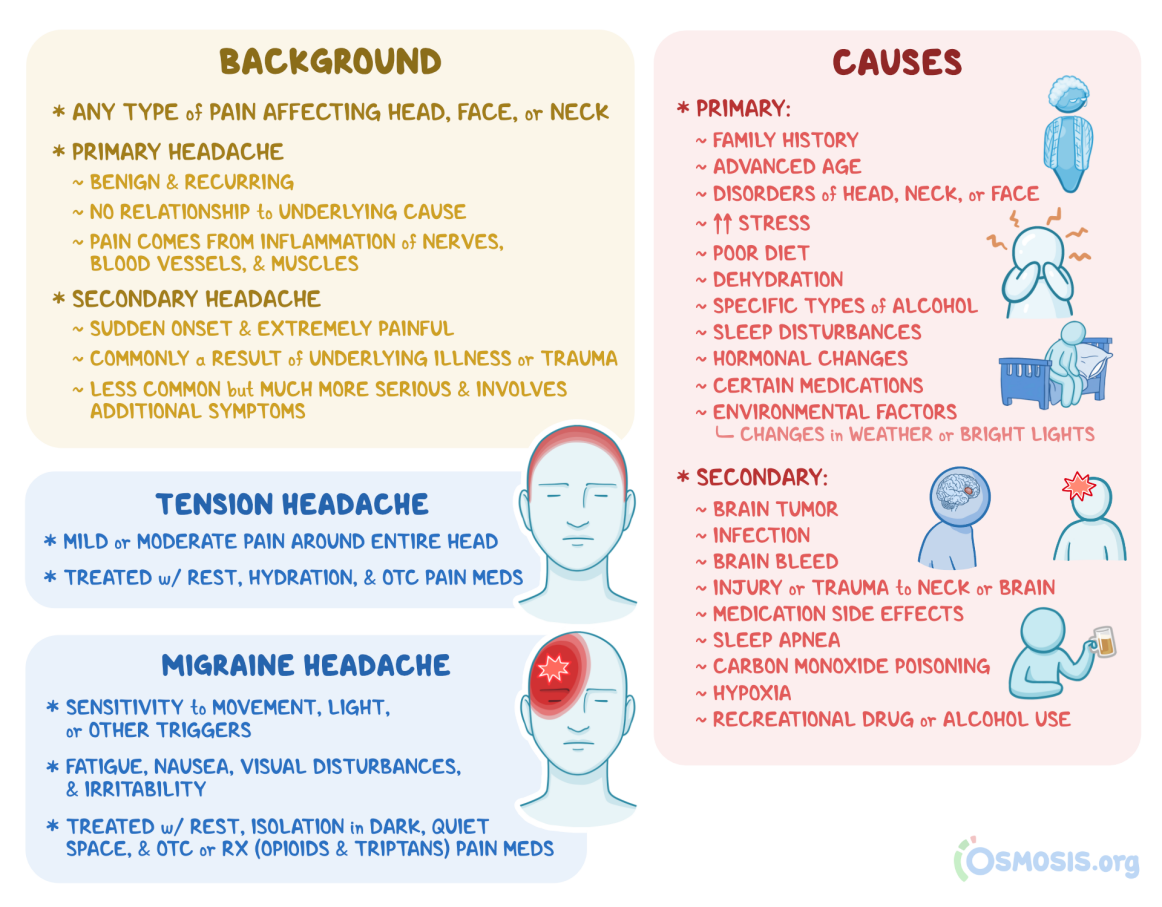
It is of outmost importance for the physician to understand the nature of the headache; whether it is primary (the symptoms arise from the disorder itself) or secondary (where the headache is caused due to any other pathologic issue, most commonly with systemic infections).
The diagnosis of headaches is made from the medical history of the patient and the clinical picture, including the evaluation of the patient’s temporal pattern of symptoms. It is advisable to perform a CT for every patient with headache complaints, in order to be sure that serious intracranial diseases like brain tumors are excluded.
There are some important points that should be evaluated in order to differentiate the type of the headache, including: the onset, the frequency and the duration of the episodes, the characteristics of pain; whether it is constant, throbbing, unilateral, like a “tight band” etc., as well as the presence or absence of aura and other accompanying features, like neck stiffness, along with other exacerbating factors including movement, light, and noise. Lastly, it is vital to evaluate the precipitating factors, such as if it is associated with the alcohol intake, menstruation, stress or even, if it is the outcome of a head injury.
The clinical examination is usually normal in patients experiencing headaches, nevertheless the physician should evaluate the level of the patient’s consciousness based on the Glasgow Coma Scale. Moreover, the doctor should seek out other focal neurological signs including papilledema, and additionally to check for signs of diseases that could affect the ears, the sinuses or that could cause restriction of the neck movements, pain in the temporomandibular joint, or thickening and loss of pulsation in the temporal arteries. Last but not least, the level of blood pressure should also be evaluated.
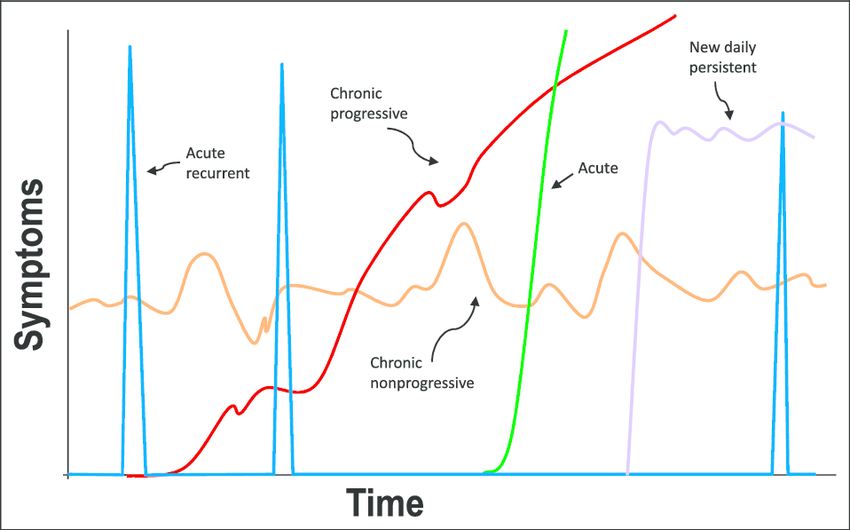
Based on the temporal patterns of symptoms, the headache types can be also classified as acute, subacute, new daily persistent headaches, episodic and chronic daily headaches. However, the most important classification categorizes the types of headaches into primary or secondary, as it is already mentioned above. In the primary headaches classification, there are three well-known types; migraines, tension-type headaches and cluster headaches.
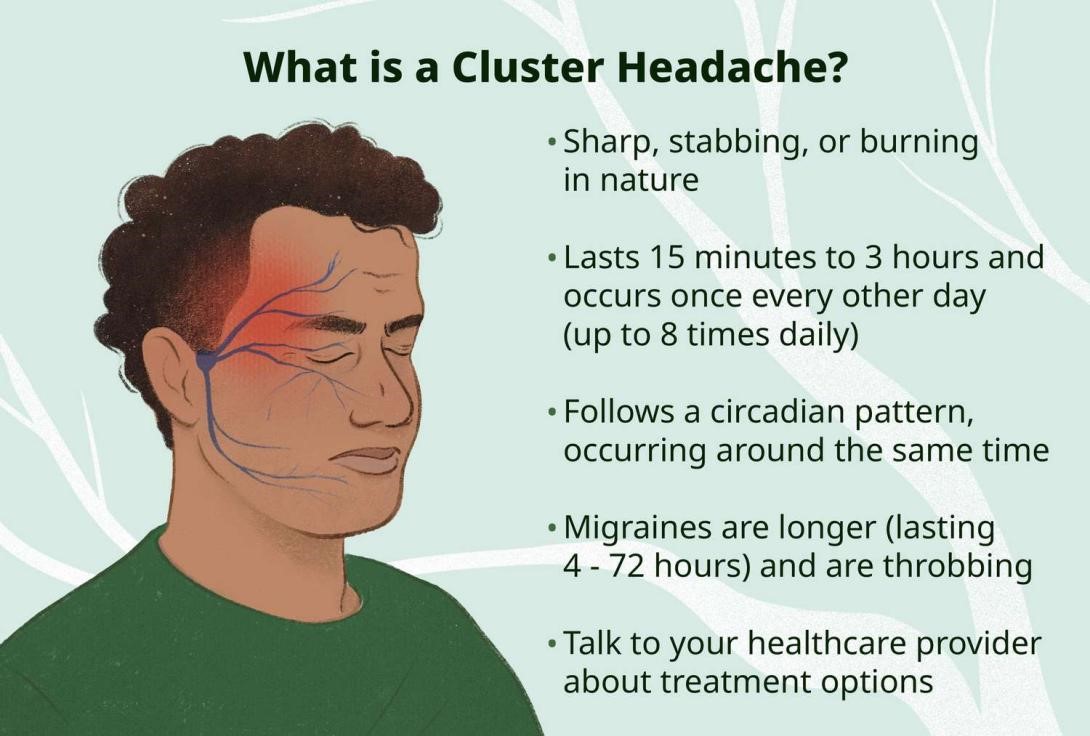
One of the aforementioned types of primary headaches is migraine. Migraine is characterized by an episodic, unilateral, throbbing pain that can last from 4 to 72 hours, affecting mostly females than males. Migraine is commonly associated with a genetic component, but still, there is the possibility of some of its rare forms to be associated with some specific mutations.
There are two types of migraines, with or without aura, where aura is an abnormal cortical electrical activity, which can be presented as visual aura, somatosensory, or motor type of aura, commonly lasting from 5 to 60 minutes. The patient may also complain of photophobia, phonophobia, and it is also possible to report nausea and vomiting. Additionally, it is also common for the patient to not be able to do anything apart from laying in a dark room until the migraine passes.
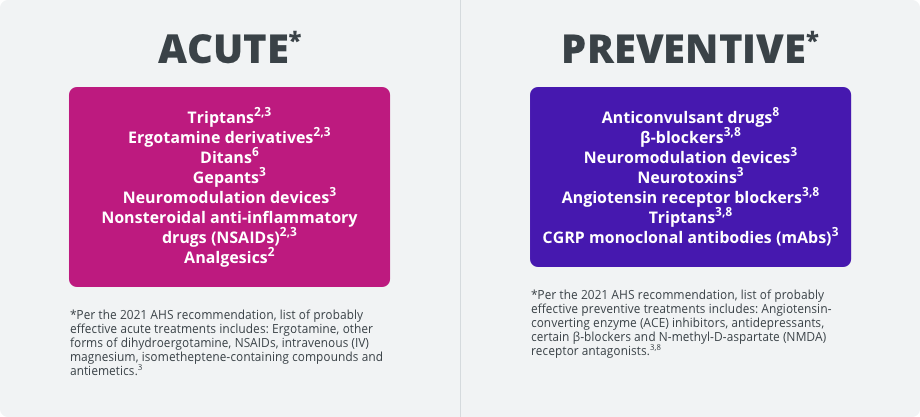
The management of migraines should exclude the presence of secondary causes and conclude that it is of primary etiology, associated with an inherited tendency. It is also crucial to advice the patient to avoid or reduce any provoking factors like stress, dehydration, and certain foods, or to improve their sleeping schedule. Furthermore, it is wise to change the drug regimen of patients suffering from migraines, especially if these patients are on oral contraceptives or on any other form of hormonal treatment.
Moreover, the individuals that suffer from migraines are advised to take analgesic drugs, such as paracetamol during an attack. Also, if the patient experiences severe attacks for more than four times a month, some prophylactic medications are indicated, including Propranolol, Topiramate or Candesartan. It is also suggested for some refractory cases of migraine, for botulinum toxin or peripheral nerve blocks to be performed.
Another type of primary headache is the tension-type headache. The main complaint is usually the diffuse, “band-like” type of pain, which can be accompanied by scalp tenderness that can last up to several hours. It can be classified as episodic, with duration lasting less than 15 days per month, or chronic, lasting for more than 15 days per month. The main type of management in the episodic tension-type headaches involves physical treatment, like massages or non-steroidal anti-inflammatory drugs, such as paracetamol, while for the chronic tension-type of headaches the treatment involves Amitriptyline.

The last type of primary headaches that will be mentioned in this article is the cluster headache. Epidemiologically, it is rare, manifesting mostly in males in their early, middle life. Its main symptoms involve a severe, unilateral pain around the eye with subsequent features, such as conjunctival injection, lacrimation and rhinorrhea. This type of headache can last up to 3 hours, while following a circadian type of pattern, occurring most frequently early in the morning, without being associated with movement sensitivity. Patients suffering from this type of headache should undergo neuroimaging, in order to exclude any pituitary pathologies.
Regarding its treatment, since its symptoms peak rapidly, it can be treated with inhalation of 100% oxygen for 15 to 20 minutes or with Sumatriptan nasal sprays. Some prophylactic methods include drugs like Verapamil (although it may cause bradycardia, therefore regular electrocardiograms are advised during the course of the treatment), Topiramate and a short course of steroids. For chronic cluster-type headaches, neuromodulation including deep brain stimulation can prove beneficial.
In conclusion, headache is one of the main disorders that millions of patients globally struggle with. There are many classification systems for the headaches, however the most common one divides them into primary and secondary types. Some of the possible accompanying features involve auras, and it is suggested for every patient with headache to undergo a CT scan, in order to exclude any malignant pathology. The aforementioned three types of primary headaches present different etiology, symptomatology and are managed differently, therefore it is advisable for every patient experiencing frequent headaches to visit their doctor in order to get examined, and subsequently to get relieved.
References
- Umesh Vivekananda. Crash Course Neurology 5th Edition. Elsevier. Amsterdam. 2019.
- Migraine and other headache disorders. WHO. Available here

