
By Frangiska Mylona,
Erectile dysfunction. Sadness, disappointment and fear accompanies impotence that can ruin a night full of expectations…
According to the International Journal of Impotence Research in 2000, it was estimated that the worldwide prevalence of erectile dysfunction is expected to increase to 322 million men by 2025. Other estimations, like the one from the Cleveland Clinic in 2019, stated that 1 in 10 men have experienced erectile dysfunction at least once in their lifetime. Having erectile dysfunction, does not mean that the definitive cause is associated with vascular diseases, since there are other etiologists, including, obesity, smoking, diabetes anti-hypertensive and antidepressant drugs, as well as, low testosterone levels and other endocrine disorders.
Nevertheless, according to the Boston University School of Medicine in 2002, studies have indicated that vascular diseases are the most common cause of erectile dysfunction with 64% of men with impotence having experienced heart attack while 57% had undergone bypass surgery. To understand the link between atherosclerosis and erectile dysfunction, is important to dig into the world of physiology and study the way an erection occurs.
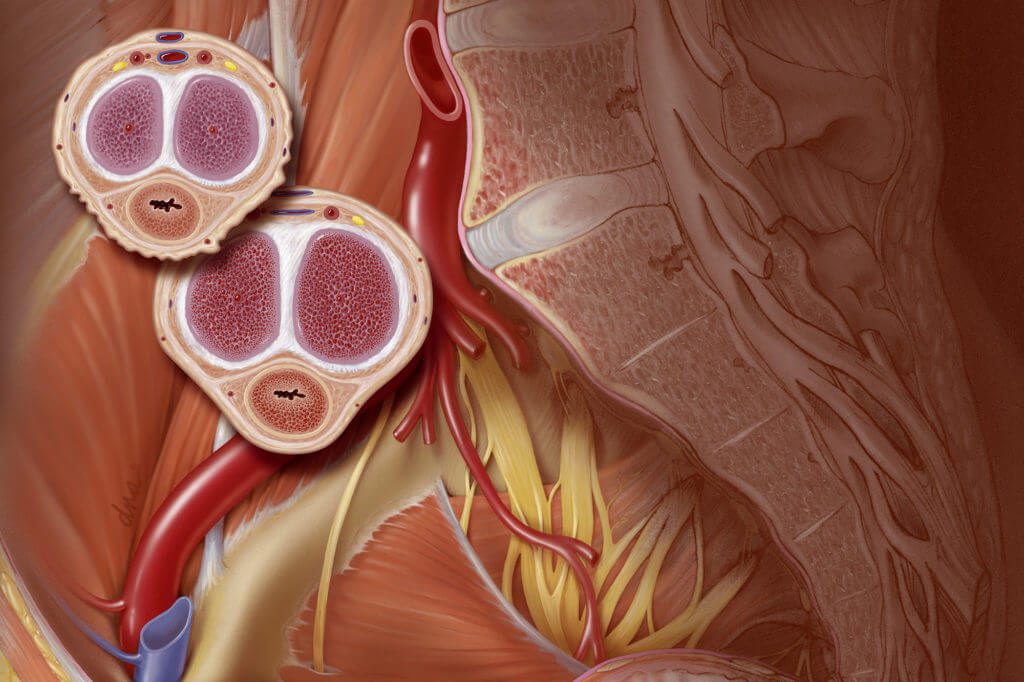
The penis along with the scrotum belong to the external male genital organs. The internal male genital organs are the testes, epididymides, ductus deferentes, seminal glands, and the prostate. In continuation, the penis has both excretory and copulative functions and it consists of 3 parts, the root, the body (shaft), and the glans. It, also, consists of three erectile bodies; the paired corpora cavernosa and the corpus spongiosum. The root of the penis is the most proximal and fixed part of the penis which is not visible externally. It is composed of the masses of the erectile bodies which are the two crurae and the bulb of the penis which are partially surrounded by two muscles; the bulbospongiosus and the ischiocavernosus muscles.
The body (shaft) is the free part of the penis which is located between the root and glans. It is the point where the bulb of the penis becomes the corpus spongiosum and the two crurae become the two corpora cavernosa, as well. Cavernous spaces are present in the two corpora cavernosa and they fill with blood during erection. It is also noticeable that the urethra passes through the corpus spongiosum.
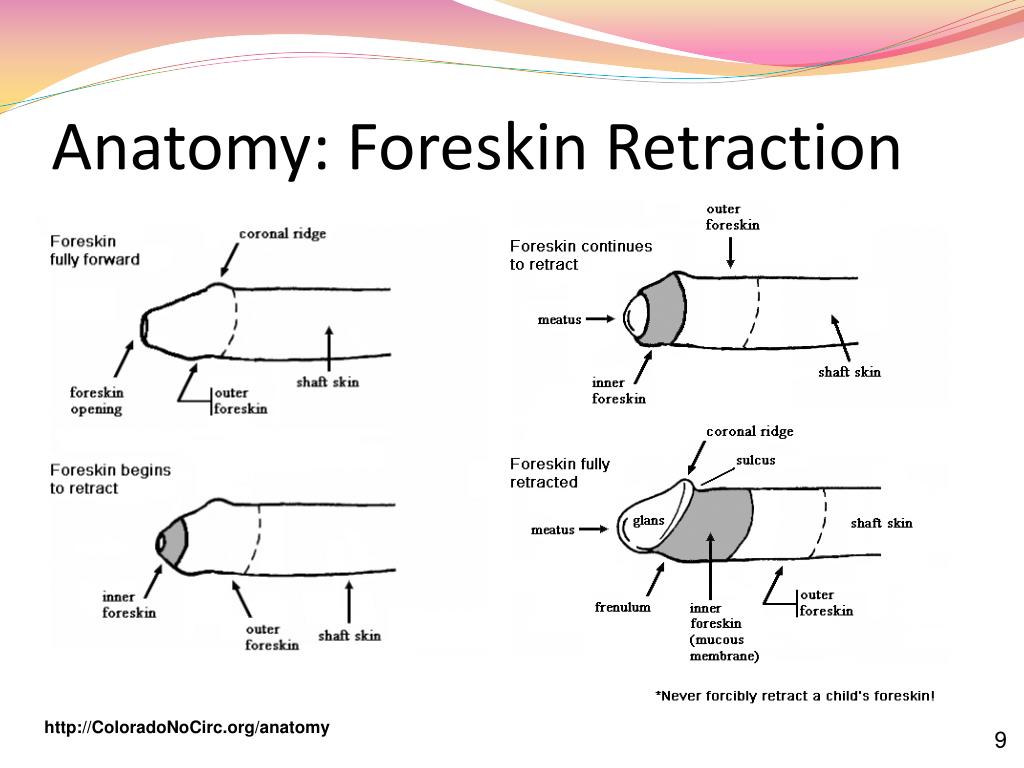
The glans are the most distal part of the penis. It is formed by the expansion of the distal end of the corpus spongiosum. The glans are covered by a skin reflected upon it known as prepuce (foreskin). The prepuce is attached to the ventral surface of the glans by the frenulum (a fold of skin that also carries a small artery). Moreover, the foreskin contains nerve endings that protect and lubricate the skin of the glans. A very familiar, and very popular surgical procedure that was greatly performed in the past, known as circumcision, removes the prepuce typically after a few days of birth. Also, the glans contains the opening of the urethra known as the external urethral orifice.
Regarding the blood supply of the penis, there are specific vessels responsible for the perfusion of each part. The crura along with the corpora cavernosa receive blood from the deep arteries of the penis. On the other hand, the bulb and the corpus spongiosum receive blood from the bulbourethral artery. Finally, the glans, the prepuce, and the skin of the penis are supplied by the dorsal artery of the penis. About the venous drainage of the penis, it is facilitated by the superficial and deep dorsal veins.
The perfusion of the penis is the first step to understand the physiology of erection. For an erection to occur, both neural, vascular as well as psychological, and endocrine factors need to work together. Erection may be the result of a cortical reaction associated with visual, auditory, or tactile stimuli or it may be a mechanical response without the need of a cortical input. Also, sleep, and particularly the REM phase, which is associated with dreaming, can induce an erection. Either way, the involvement of the parasympathetic nervous system is the one responsible for triggering an erection by increasing the circulating nitric oxide.
Nitric oxide acts as a vasodilator, causing the corpora cavernosa to fill with blood and engorge. Adding to that, the two muscles that partially surround the bulb and the crura; the ischiocavernosus and the bulbospongiosus muscles, will compress the veins of the corpora cavernosa, preventing the blood’s backflow and therefore maintaining the erection. Depending on the flaccid dimensions of a penis, it can increase in size during the erection with its average length to be measured around 15 cm.
Ejaculation is the usual outcome of an erection. Ejaculation is controlled by the sympathetic nervous system. Also, the glans of the penis can play an important role, since it has high concentrations of nerve endings that can influence the likelihood of ejaculation. By understanding the importance of the blood supply for an erection, is easy to connect erectile dysfunction with atherosclerosis and with vascular diseases in general.
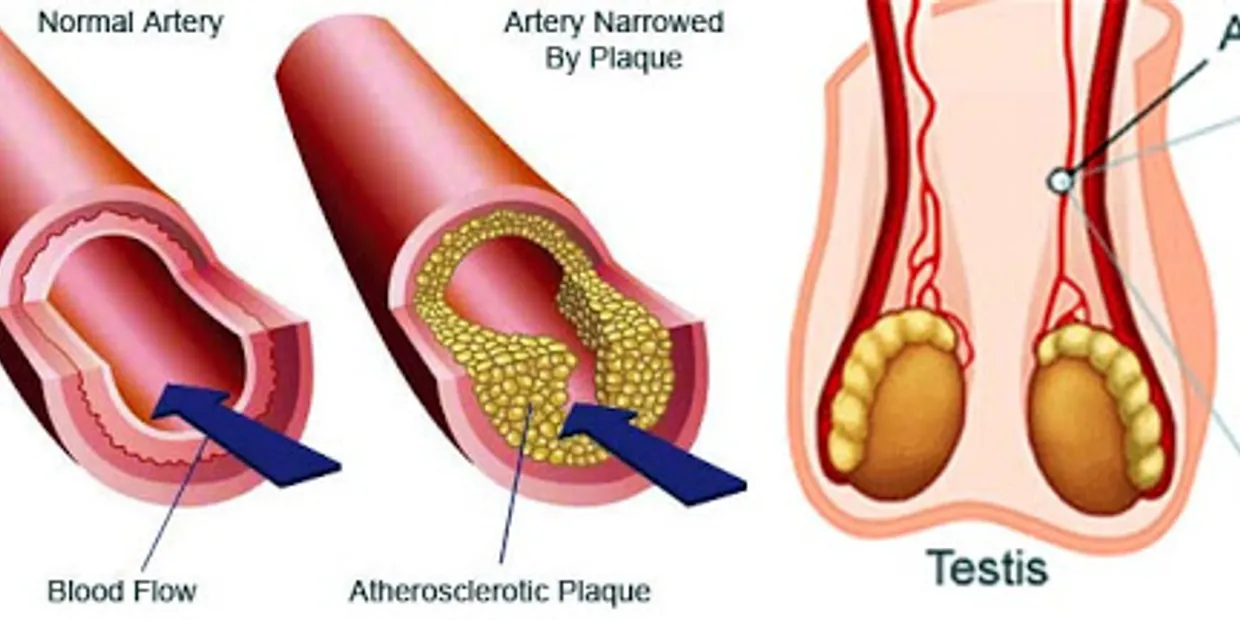
Atherosclerosis is a familiar term referring to a common vascular disorder characterized by lipid deposition in medium and large-sized arteries leading to their intimal thickening. This progresses in steps where the first step is the formation of fatty streaks.
Fatty streaks are associated with endothelial dysfunction due to various risk factors like tobacco or hyperglycemia causing the endothelium of the arteries to have lower defenses against lipid deposition. This endothelial dysfunction allows LDL (known as “bad” cholesterol) to be deposited under the endothelium of the arteries. In the later stages, macrophages “eat” the LDL cholesterol particles, and as a result, they get stuck and transformed into foam cells. This deposition will eventually lead to plaque formation that will ultimately narrow the affected artery.
At this stage, plaque has two pathways of progression. It can either be stable causing chronic ischemia or it may become vulnerable resulting in thrombosis or embolization. The complications of atherosclerosis, apart from erectile dysfunction, involve aneurysm formation, ischemia, and clots which can progress to a myocardial infraction, or even, stroke.
It is needed to be understood that any vessel can get affected by atherosclerosis even the arteries that are responsible for the arterial blood supply of the penis. Thus, it is concluded that atherosclerosis can cause a reduction in the blood flow that is needed for an erection. Moreover, in normal conditions the endothelium of the vessels is protected by nitric oxide against lipid deposition, therefore, when there is endothelial dysfunction, it can disturb the relations with the nitric oxide resulting in reduced protection against lipid deposition.
To dig more into the relationship between impotence and atherosclerosis, it is needed to mention that size matters when it comes to arteries. For example, the coronary arteries (responsible for the heart’s arterial blood supply) have a much larger sizes than the penile ones, therefore the same level of atherosclerosis will cause a significantly more blood flow reduction in the penis when compared to the coronary circulation.
Harvard’s Medical University named the erection as the “barometer of the overall health in males” and it is true, because erectile dysfunction may prove to be an alarming symptom. A study made by Montorsi et al. examined a group of 300 men that were affected by significant coronary artery disease, to assess the prevalence of erectile dysfunction among them. The results showed that almost half of the patients have experienced erectile dysfunction. This study along with others, set the conclusion that erectile dysfunction might be the alarming sign of a cardiovascular disease that silently and slowly progresses.
If there is a suspicion that atherosclerosis or other cardiovascular diseases are responsible for the patient’s erectile dysfunction, the therapeutic approach is versatile. The first steps involve adopting a healthier lifestyle, by reducing smoking and losing weight, as well as following a healthier diet. Also, medications can be proven helpful like, the very famous, Viagra (Sildenafil) that stimulates an erection (although prior discussion with a doctor as well as thorough analysis of the patient’s medical condition, medical history, and medication regimen needs to be assessed before its administration). New research programs aimed at improving the therapeutic approach, are focusing on the use of oral hypoglycemic drugs in diabetic patients with erectile dysfunction.
In conclusion, erectile dysfunction is not mandatory associated with atherosclerosis or other cardiovascular diseases, however, one must consult a doctor if they experience erectile problems. This association of impotence and atherosclerosis, is an example of the way that the body “alerts” the patient that something malfunctions. It is better to prevent than treat a disease and doctors are always there to save one’s night and, maybe one’s life.
References
- Endothelial Dysfunction, Erectile Deficit, and Cardiovascular Disease: An Overview of the Pathogenetic Links. Available here
- Crash Course edition 5th, Anatomy and Physiology by Samuel Hall, Jonny Stephens.
- Crush Step 1, 2nd edition, The Ultimate USMLE Step 1 Review by Theodore X.O’Connell, Ryan A.Pedigo, Thomas E.Blair.

