
By Frangiska Mylona,
The GOLD standard for diagnosing ulcerative colitis includes biopsy and colonoscopy. As for the radiological CT findings in ulcerative colitis, the thickening of the bowel wall is visible with irregular narrowing of the bowel’s lumen and infiltration of the surrounding fat. However, this radiological image could be found in other causes of colitis, therefore clinical and medical history are of great importance.
Differential diagnosis refers to the different diseases that have the same symptomatology. For example, regarding Crohn’s disease, celiac disease can mimic symptoms of pain and malabsorption. Acute fever with right lower quadrant pain also resembles appendicitis. Moreover, fever, pain, weight loss, and abnormal small bowel radiography can be seen in intestinal lymphoma. Patients prescribed NSAID drugs can be affected by NSAID-induced colitis.
The initial representation of ulcerative colitis is almost identical to other causes of colitis. Infectious colitis must be excluded by testing for Salmonella, Shigella, and amebiasis. In immunocompromised patients, cytomegalovirus (CMV) colitis can be mistaken for ulcerative colitis. Sexually transmitted diseases like gonorrhea or chlamydial infections should be considered in active sexual patients with proctitis. Lastly, patients prescribed corticosteroids can also be affected by CMV colitis. Complications refer to a secondary disease or condition that worsens the already existing one. In Crohn’s disease, possible complications include abscesses, small bowel obstruction as well as fistula formations in the abdomen or the rectovaginal space as well and perianal diseases. Also, the already mentioned malabsorption syndromes including vitamin B12 deficiency that can lead to anemia should be considered in Crohn’s disease.
In ulcerative colitis, complications may include an increased risk of developing colorectal cancer, toxic megacolon, osteoporosis, primary sclerosing cholangitis, and fulminant colitis. Last but not least, IBD can deteriorate the psychological status of the patient resulting in anxiety and depression. Psychological treatment like cognitive behavioral therapy could be effective, however, there is limited scientific data to this day to prove it.
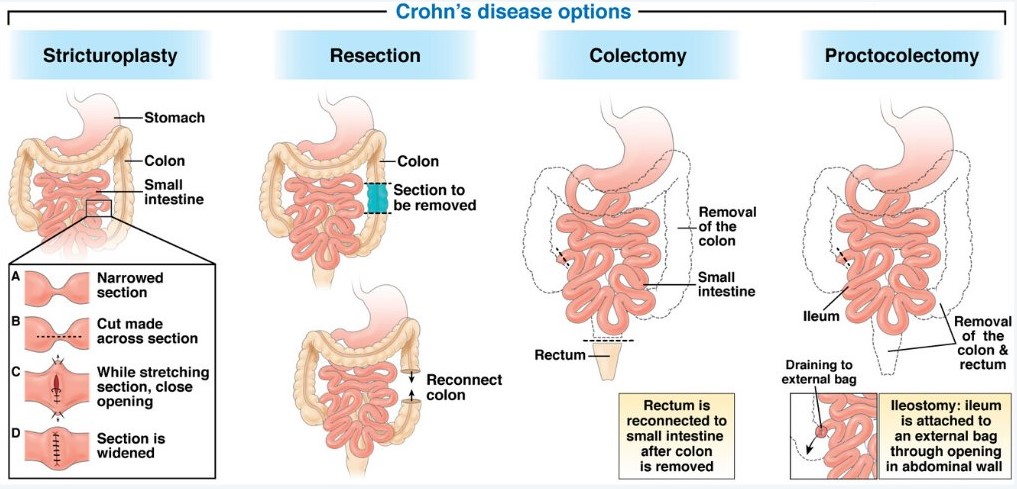
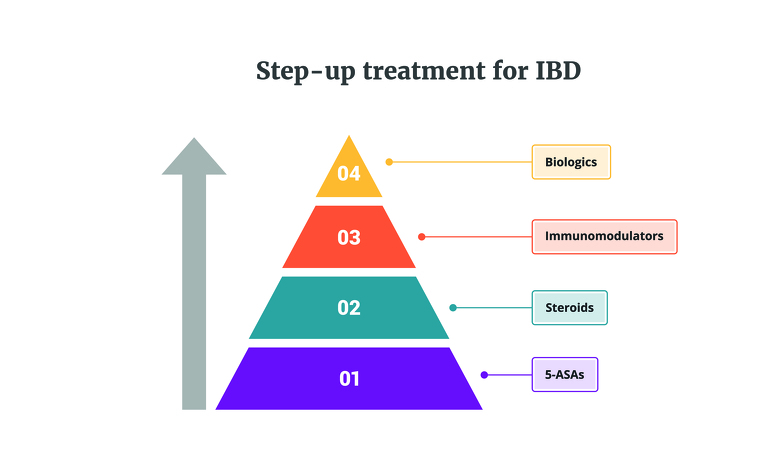
Although ulcerative colitis and Crohn’s disease are two different pathologies, several pharmacologic agents can be used to treat both. The main elements of treatment include 5-aminosalicylic acid derivatives (5-ASA, although they are not completely effective for Crohn’s disease and they are used only in mild cases and in conjunction with other drugs), corticosteroids, thiopurines, biological therapies, dietary changes, and surgery. It is important to outline that surgical treatment is not curative in Crohn’s disease and it is performed only for complications and for symptom alleviation.
On the other hand, in ulcerative colitis, surgical procedures are usually curative. When patients suffer from chronic obstructive symptoms due to short ileal stenosis in Crohn’s disease, they can be treated with resection or stricturoplasty. Other indications for surgery include intra-abdominal abscesses, massive bleeding, or perianal fistulas. In ulcerative colitis, indications for surgery include severe hemorrhage, perforation, or documented carcinoma. Surgery is also indicated for fulminant colitis and toxic megacolon that does not improve within 24-28 hours
Biological therapies target many components of the immune system and they are very effective for patients suffering from moderate to severe disease. When they are administered early in the disease, they can improve its natural progression. However, both their expensive cost and their potential harsh side effects should be considered. These therapies include anti-TNF therapies, anti-integrins, anti-IL-12/23 and anti-IL-23 antibodies.
Inflammatory bowel diseases can pose both physical and psychological challenges, so improving lifestyles and establishing healthier habits can lead to a better prognosis and a better outcome as well as a reduced mortality rate, particularly when it comes to Crohn’s disease. Among these changes are the cessation of smoking and the limitation or reduction of alcohol consumption. Engagement in physical activities should be encouraged as well as the modification of dietary habits. Diets low in saturated fats and red meat, with plenty of fruit and vegetables are recommended for patients without intestinal strictures. A classic example of these diets is the Mediterranean diet.
It is important to consider that vaccination status should be checked in all patients affected by inflammatory bowel diseases. Inactivated vaccines for hepatitis A and B, vaccines for herpes zoster, and influenza as well as the DTaP vaccine for tetanus, diphtheria, and pertussis can be safely administered in patients receiving immunomodulator therapy. However, live virus vaccines should be given to unvaccinated patients before being administered immunomodulator therapy but, under no circumstances, should they be administered when the patient is under immunosuppressive treatment. In conclusion, with proper medical and surgical treatment, most of the patients will be able to cope and succeed in their everyday life. Compliance with the treatment as well as a supportive environment, can help the patient to thrive and succeed in the challenges of everyday life.
References
- CURRENT Medical Diagnosis & Treatment, 2024, edited by Maxine A. Papadakis MD, Stephen J. McPhee MD, Michael W.Rabow MD, Kenneth R.McQuald MD. Associate editor Monica Gandhi MD, MPH. Sixty-third edition.
- Davidson, Παθολογίας; Γενικές αρχές και κλινική πράξη της Ιατρικής ,22η Έκδοση/ 5η Ελληνική Έκδοση, Επιστημονικές Εκδόσεις Παρισιάνου Α.Ε.
- Learning radiology, recognizing the basics, 5th Edition by William Herring, MD, FACR
- Ulcerative Colitis Imaging; Available here

